Chronic ankle instability (CAI) is an ongoing ankle condition, typically persisting after an initial injury affecting the structures that support the ankle. Because the foot and ankle complex forms the foundation for most physical activities, CAI can dramatically impair athletic performance, reduce overall mobility, and increase the risk of additional injuries. Without successful rehabilitation, compensation patterns that alter biomechanics can take a toll on structures and tissues throughout the body.
When faced with the challenge of restoring ankle stability, many doctors and therapists are ill-equipped to achieve optimal results due to lack of knowledge and resources. At NYDNRehab, we leverage advanced technologies, orthobiologics, and cutting-edge therapies to rehabilitate damaged ankles and restore functional stability. Our track record of CAI success, backed by 20+ years of experience, makes NYDNRehab the clinic of choice for ankle rehabilitation in NYC.

Clinical director & DC RMSK
Verified Expert Profiles

Dr. Lev Kalika, DC clinical director and founder of NYDNRehab, is an internationally recognized expert in diagnostic and musculoskeletal ultrasonography, with multiple research publications to his credit. Dr. Kalika has studied alongside some of the world’s most prestigious experts in diagnostic, fascial, and nerve ultrasonography, and has presented his research at multiple international conferences.
Dr. Kalika was among the first in his field to become certified in Dynamic Neuromuscular Stabilization (DNS), one of the most evidence-based approaches for treating chronic ankle instability. Dr. Kalika was mentored directly by the creator of DNS, Dr. Pavel Kolar.
Dr. Kalika is an active member of the American Institute of Ultrasound in Medicine (AIUM), and has developed his own unique approach to Dynamic Functional and Fascial Ultrasonography. His expertise in human anatomy and biomechanics, coupled with his skills in interpreting high-resolution ultrasound imaging, means patients at NYDNRehab get a comprehensive and accurate diagnosis that translates to successful treatment.

Orthobiologic, Sports Medicine and Regenerative Medicine Specialist
When it comes to complex post-traumatic ankle pain and instability, most medical doctors are at a loss for how to successfully restore ankle function. Attempts at orthobiologic injections and physical therapy may be provided, based on MRI imaging, but MRI cannot capture the many nuances of ankle injuries involving multiple structures and tissues. When attempts at ankle rehab fail, patients are often referred for surgery, but surgical interventions do not guarantee satisfactory outcomes, and surgery may even worsen ankle instability.
At NYDNRehab, we use the highest-resolution diagnostic ultrasonography to dynamically visualize your ankle in real time. Ultrasound gives us insight into impaired ankle biomechanics that cannot be detected by MRI, helping us to discern which structures can benefit from orthobiologics, regenerative technologies, and targeted physical therapy.

Dynamic high-resolution ultrasound imaging has multiple advantages over MRI:
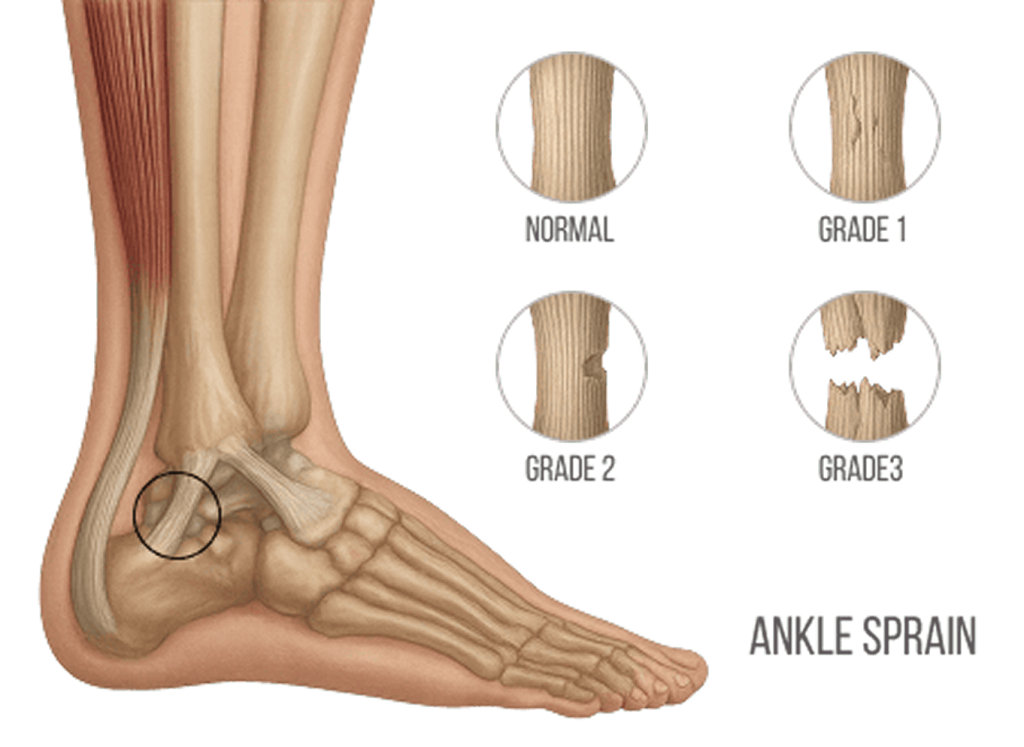
Structural instability typically features damage to ligaments, most often due to a lateral ankle sprain. By contrast, functional instability is often caused by deficits in proprioception (sense of joint position), neuromuscular control (ability of muscles to react quickly), and balance, often stemming from previous ankle sprains.
Differentiating between structural and functional instability is a critical step in developing the most effective treatment protocol – a distinction that most doctors and therapists are unequipped to make, often resulting in unnecessary surgeries that fail to restore ankle stability and function.
Prior to beginning physical therapy, we pretreat your tissues to restore their functional properties, and retrain neuromuscular pathways that have been disrupted by your injury. Even old injuries can be successfully rehabilitated, and persistent compensation patterns can be eliminated. We take into account muscles, connective tissues, fascia, nerves and blood vessels whose functional properties have been altered due to injury.
At NYDNRehab, we never rely on one-size-fits-all treatment protocols that fail to deliver results. Our CAI therapy is not isolated to your ankle – in most cases of CAI, functional biomechanics are altered along the entire lower kinetic chain, requiring corrective measures to restore optimal mobility and performance. Our personalized holistic approach to patient care means you get customized treatment based on your unique patient profile.

Due to the complex structural architecture of the foot and ankle, multiple factors can play into ankle instability, and no two injuries are exactly alike. Symptoms-based diagnosis can help identify the problem, but it cannot factor in the many individual nuances that contribute to ankle instability.

CAI typically arises after an initial ankle sprain, frequently involving the lateral ligaments. If not properly rehabilitated, ankle instability can have major downstream effects that affect biomechanics throughout the body. Conventional efforts at rehabilitation often stop once ankle pain subsides, leaving the patient with ongoing issues that reduce overall mobility and performance.
In addition to a history of recurrent ankle sprains, multiple other factors can increase the risk of developing CAI.
In general it is not difficult to identify an unstable ankle, but naming the condition is not enough to successfully treat it. In most cases, patients with CAI have suffered repeated sprains, doing damage to multiple tissues and structures that make up the ankle complex. Unless all damaged tissues are identified and healed, physical therapy alone is unlikely to restore ankle stability.
Many doctors rely on MRI to visualize injured tissues, and some may even administer advanced treatments like orthobiologics and shockwave therapy. But MRI can overlook subtle damage to ligaments that affect ankle function, and MRI cannot single out other factors like impaired proprioception, fascial dysfunction, muscle weakness, and balance issues.
Moreover, CAI often causes compensation patterns that affect alignment and function along the entire kinetic chain. Treating the ankle alone without addressing other factors is bound to deliver suboptimal results, and may even make matters worse.
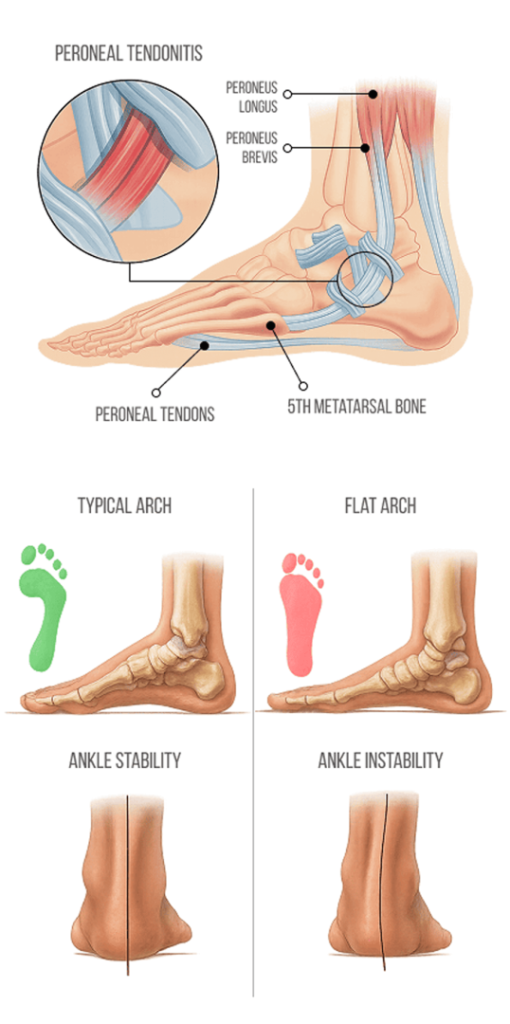
A recent review of studies found evidence that Individuals with CAI exhibit multiple motor control abnormalities, with alterations in the tibialis anterior muscle on the front of the shin, and the peroneus longus muscle that dorsiflexes and inverts the foot – muscles critical for ankle stability. The subjects also exhibited premature activation of the hip and spinal muscles before activation of the ankle muscles.
In a recent cross-sectional study, researchers used EMG to assess muscle activation in terms of amplitude, to compare participants with unilateral CAI to an uninjured control group. Both groups walked on a split-belt treadmill, with and without random left- and right-sided perturbations. Results showed that the CAI group had altered bilateral motor control strategies, with earlier activation of the leg muscles (rectus femoris, biceps femoris, and gluteus medius), along with premature activation of the trunk muscles (bilateral rectus abdominis and non-erector spinae) compared to the control group.
Another controlled study compared a CAI group to uninjured participants using cutting and landing tasks. The CAI group exhibited smaller dorsiflexion angles in the landing tasks, with greater foot eversion, and reduced foot stability. The researchers suggested that these factors should be considered when designing and implementing interventions to restore ankle function in CAI patients.

Attempting to treat the ankle without addressing biomechanical abnormalities is a recipe for failure. At NYDNRehab, we treat the whole patient, not just the site of injury. To get the big picture, we conduct a thorough in-office exam on your first visit, using high-resolution diagnostic ultrasound to visualize your injury in real time. Dr. Kalika’s in-depth knowledge of human anatomy and his expertise in diagnostic ultrasonography ensure that all damages from your injuries are identified and taken into account when designing your personalized treatment plan.
In addition to diagnostic ultrasound, we conduct gold-standard assessments to establish a baseline of ankle function, giving us objective metrics for measuring your progress.
Your functional ankle assessment may include a battery of some of the following:
Once we have an overall profile of the extent of your injuries, we design a personalized treatment plan based on your results. Our holistic approach ensures that all factors contributing to your ankle instability are addressed, resulting in superior outcomes compared to conventional treatment and surgery.
The human ankle is remarkably strong, able to withstand forces 4-5 times a person’s body weight during running and jumping activities. The foot and ankle complex provides a solid base of support for the entire body, relying on proprioception to make subtle changes in position to maintain balance. Proprioceptors in the foot and ankle allow for adaptation to changes in terrain, and rapid responses to outside forces.
There are multiple structures that contribute to ankle stability, but the majority of support is provided by the lateral and medial ligaments. On the medial (inner) side, four ligaments create a fan-like pattern – the anterior tibiotalar, posterior tibiotalar, tibionavicular and tibiocalcaneal ligaments – collectively referred to as the deltoid ligament.
On the lateral (outer) side, the ankle is supported by three primary ligaments – the anterior talofibular, posterior talofibular, and calcaneofibular ligaments. The lateral ligaments are not as strong as the deltoid ligament, and are at higher risk of injury. The peroneal muscles provide additional lateral stability, helping to prevent excessive inversion of the ankle.
The critical role of fascia in ankle stability has only recently been recognised by researchers, and many conventional practitioners are not aware of its importance in ankle structural integrity. Fascia acts as a stabilizing framework throughout the body, holding muscles, connective tissues and organs in place, preventing excessive movement, and maintaining joint alignment during dynamic activities.
Fascia promotes ankle stability by providing structural support, contributing to force transmission, and delivering proprioceptive feedback. Fascial tissue has a significantly higher density of proprioceptors (sensory receptors) compared to muscle tissue, making it more sensitive to changes in pressure, stretch, and movement, and serving as a prime source of information about the position of the lower kinetic chain.
Fascia and muscles work synergistically to guide and control movement, and to mediate internal and external forces – a concept called biotensegrity. Healthy fascia is smooth, elastic and slippery, but when damaged, fascia can become dense and sticky, losing its elastic properties and suppressing proprioception. Fascial dysfunction can have a dramatic impact on ankle stability, and failure to treat fascia as part of the rehabilitation protocol can undermine the success of treatment.
A 2021 study of athletes with recurring ankle sprains found that the Stecoo method of fascial manipulation, in which Dr. Kalika is trained and certified, significantly improved ankle function and range of motion in individuals with chronic ankle instability.

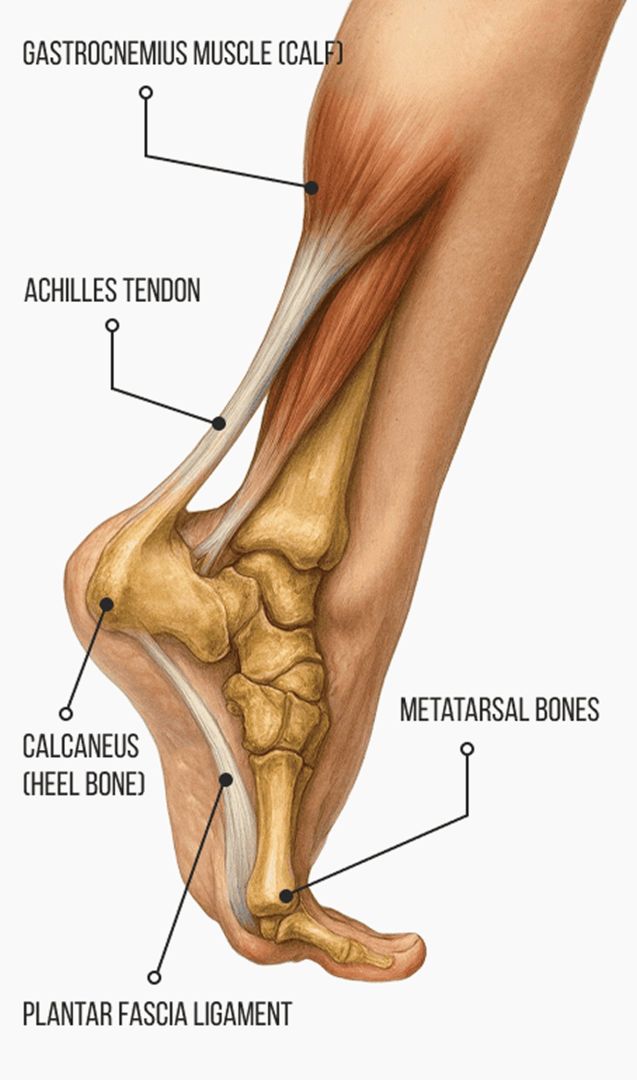
At NYDNRehab, we always begin with a conservative approach to plantar fasciitis treatment, but the secret to our success is precision. We have a 100% track record of success in treating plantar fasciitis, thanks to the combination of extracorporeal shockwave therapy (ESWT) and ultrasound guided dry needling (USDN).
A recent research publication in Nature cites Dr. Kalika’s own research, highlighting USDN as a top-tier evidence-based solution for plantar fasciopathy, and ranking it alongside ESWT and PRP as a primary intervention. To quote the article:
Current therapeutic approaches for plantar fasciopathy include targeted mechanotherapy, optimized ESWT protocols, ultrasound-guided delivery of orthobiologics (e.g. leukocyte-rich PRP), and precision physical therapies. Furthermore, studies demonstrate the diagnostic and therapeutic value of ultrasound elastography and US-guided interventions for pain modulation. Ultrasound-guided dry needling of myofascial trigger points has been established as a primary intervention option for plantar fasciopathy.”
For patients, our multimodal approach to plantar fasciitis means quick pain relief, fast recovery, and longer-lasting outcomes. In our experience, combining modalities with precision guidance creates the best results.

Conventional treatment of CAI typically involves passive interventions like taping and bracing, and active interventions such as physical therapy and balance training. But such interventions do not address myofascial dysfunction and proprioceptive deficits, and athletes are often released prematurely to sports, setting them up for more injuries.
At NYDNRehab, we pretreat damaged tissues to accelerate healing and restore biotensegrity before introducing weight-bearing activities.
We monitor your response to prehab with high-resolution ultrasound, to ensure all interventions have their intended effects. Once we are satisfied that your ankle tissues are ready to tolerate force loads, we can begin a progressive protocol of personalized, one-on-one physical therapy.
Orthobiologic injection therapies use natural/neutral solutions, injected with precision thanks to ultrasound guidance. The injected solutions stimulate cellular repair by either nourishing or irritating the targeted cells. However, orthobiologics are not a stand-alone solution – they only address tissue biology, but cannot restore functional mechanics.
Full rehabilitation of an unstable ankle requires restoration of biotensegrity, tissue strengthening, and retraining of neuromuscular pathways to optimize muscle recruitment patterns that have been disrupted. Orthobiologic treatment results are dramatically enhanced when tissues are pre-treated with focused extracorporeal shockwave therapy (fESWT) and myofascial release techniques.






Dr. Kalika’s expertise in diagnostic ultrasound combined with Dr. Brosgol’s skill in needling procedures ensure that your orthobiologic therapy has maximal impact on the targeted tissues. Once the treated tissues have healed enough to tolerate loads, we begin a progressive program of personalized physical therapy aimed at optimizing ankle mechanics.

Ankle sprains are one of the most common athletic injuries, with estimated incidence ranging from 2 to 5 per 1000 in high intensity sports involving running, jumping and cutting. Athletes often ignore mild to moderate sprains, continuing to play once the initial pain subsides. But absence of pain does not mean your ankle is healed. Failure to completely rehabilitate a sprained ankle before returning to play can mean more injuries that undermine ankle stability and reduce athletic performance.
Conventional CAI treatment by medical doctors and orthopedists does not address the many nuances of ankle instability, and surgery has inherent risks, with no guarantee of success. If your goal is to return to play at pre-injury performance levels, you need full-spectrum ankle rehab that addresses all factors contributing to CAI.
At NYDNRehab, our integrative approach, advanced methodologies, and years of experience ensure that your ankle is strong, stable and mobile, so you can return to play with confidence. NYDNRehab is your one-stop-shop for advanced diagnostics, orthobiologics and regenerative therapies, for the best functional ankle rehabilitation in NYC.





Independent peer-reviewed research relevant to this treatment approach.

Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination




















