Running is a natural human movement for which the body is well designed. From hips to toes, every joint in your lower extremities is involved in running, each absorbing its share of the workload. Running is beneficial for a broad range of health markers, including cardiovascular health, bone mineral density, weight management and healthy joints. However, running with knee pain can lead to serious injury that eventually terminates your running career.
The growing popularity of recreational running in the 1970s and beyond raised concerns about the deterioration of knee joints and the risk of osteoarthritis as runners aged. However, statistics and years of research have proven the opposite to be true. Older patients with knee osteoarthritis rarely have a past history of running. In fact, when the joint is healthy, running can be beneficial for the knees, stimulating the production and repair of cartilage, and reducing the risk of osteoarthritis later in life.
Nevertheless, high impact forces during running can cause wear and tear on your knee joints, especially if your gait mechanics are off. During the running gait cycle, ground reaction forces can increase by up to 250% of your body weight. With inefficient gait mechanics, the knees in particular are prone to injury, making knee pain one of the most common complaints among runners.
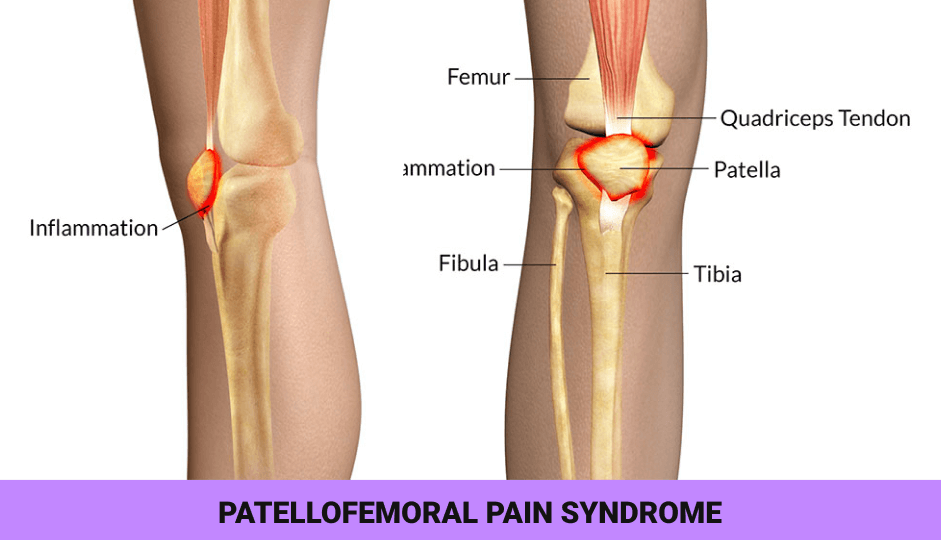
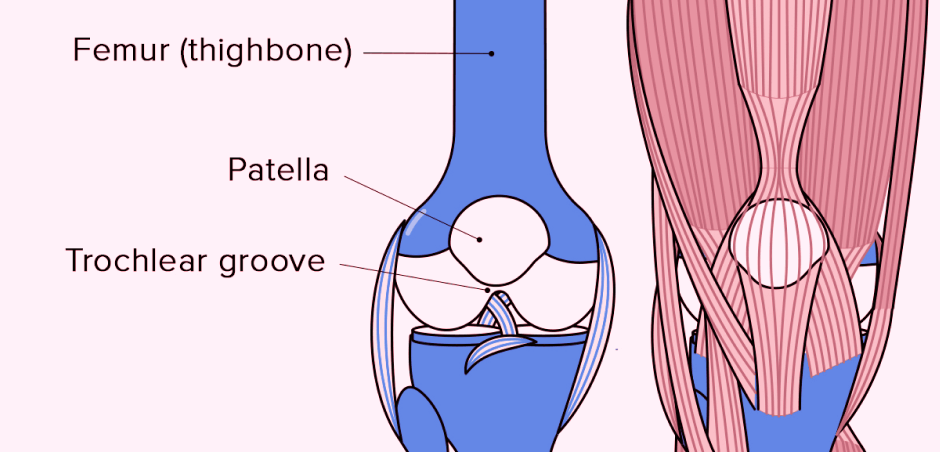
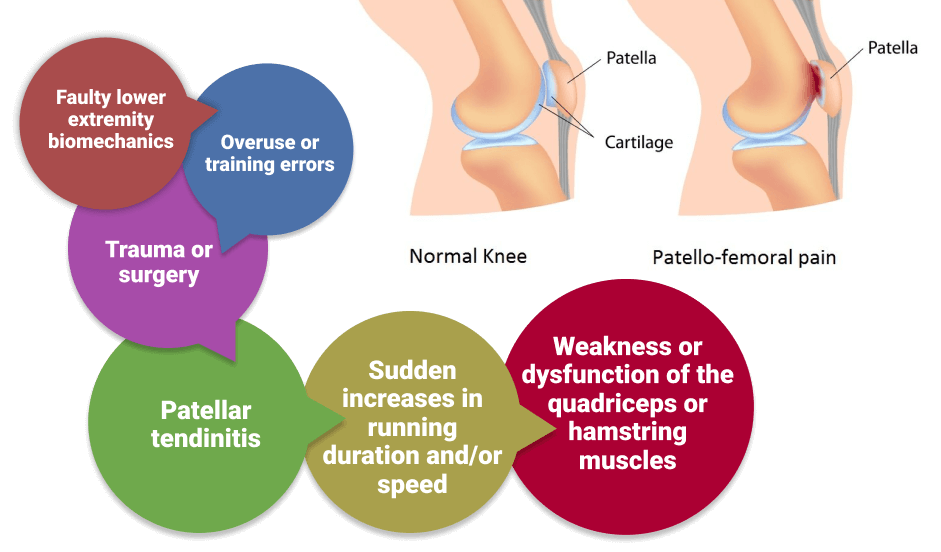
Runner’s knee, clinically known as patellofemoral pain syndrome (PFPS) is an umbrella term for anterior knee pain in physically active populations, especially runners. PRPS is caused by imbalanced forces during knee flexion and extension while the joint is loaded, preventing the patella, or knee cap, from tracking efficiently across the femur, or thigh bone.
Symptoms of PFPS include:
PFPS accounts for 16 to 25 percent of all running injuries, and the condition is more common in female runners than in males. If your knee is in pain after running, you may need to correct your running gait.
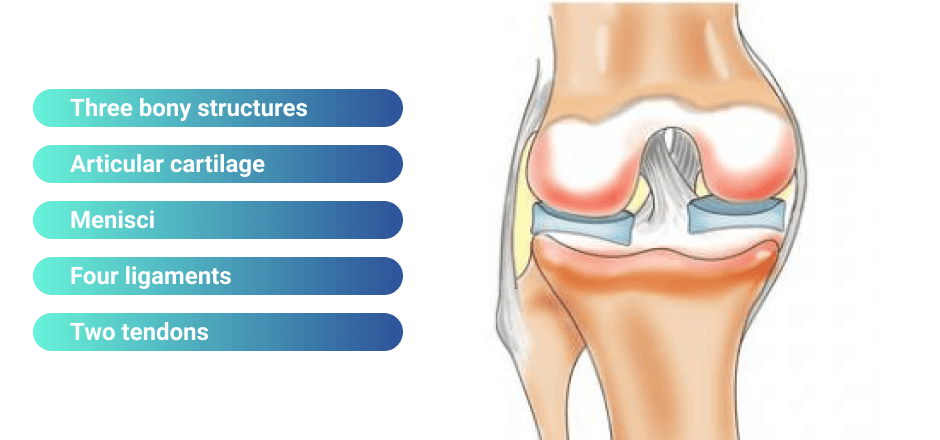
The knee is a complex joint, with many converging structures that contribute to its stability and function.
Structures of the knee joint include:
PFPS appears gradually over time, often resulting from bad habits that begin early in a runner’s career. Early detection of gait deficiencies can help runners avoid knee pain and injury, and prolong the enjoyment of running throughout an active lifespan.
Some common causes of knee pain include:
Many of the issues contributing to PFPS can be identified and corrected with a thorough and well-designed gait analysis and retraining program.
You can think of your body as a human machine, with bones acting as levers that rotate around joints serving as fulcra. Your machine is powered by muscle contraction that causes tendons to pull on bones, creating motion. Your ligaments provide a support system that holds your bones in place, while menisci, cartilage and bursa pads absorb shock and keep things running smoothly. Your knee joints are also surrounded by a synovial membrane that secretes fluid to keep everything lubricated.
Walking and running recruit the same muscles for locomotion, but compared to walking, running requires more balance, greater strength and a wider joint range of motion. During walking, at least one foot is on the ground at all times, and both feet are in contact at one point in the gait cycle.
During running, only one foot comes in contact with the ground at any time, with an airborne period during each cycle where both feet leave the ground. Propelling your body off the ground requires more muscular strength, and the range of joint angles at your ankles, knees and hips is greater for each stride compared to walking.
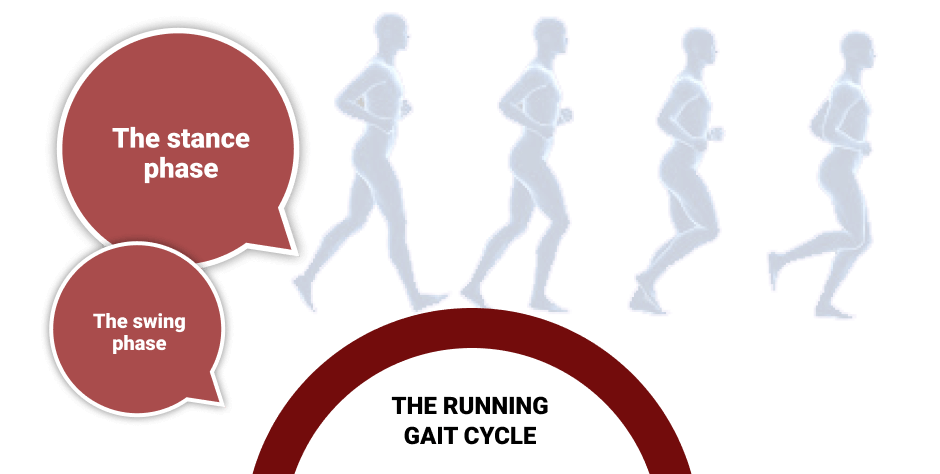
The running gait cycle consists of two phases:

Poor gait mechanics is a primary contributor to knee pain. In many cases, it stems from habitual compensation patterns formed over time that cause poor distribution of impact forces across the lower kinetic chain. Most imbalances cannot be detected by the naked eye, and require a comprehensive gait analysis using sophisticated technology.
Following are some common mechanical running errors and tips on how to avoid them:
Errors in running stride: A too-long or too-short stride can reduce running efficiency, overloading joints and burning excess energy. To improve stride:
Errors in joint angles: Failing to flex and extend the joints appropriately throughout the gait cycle can reduce running efficiency and increase the risk of injury.
Your ankle should dorsiflex as it enters the stance phase to ensure proper landing and to control your foot placement as it makes contact with the ground.
Your knee should bend slightly during the stance phase to help absorb ground reaction forces when landing, and to prepare for propulsion.
Allow your heel to float up during the swing phase, to reduce hip flexor torque.
Do not overly flex your hip in the swing phase; keep knees low toward the ground.
Errors in timing: Timing errors have to do with muscle activation patterns. If certain muscles fire too soon while others are delayed, it can result in faulty mechanics that lead to injury. Timing sometimes varies between right and left sides, creating an imbalanced stride that reduces performance. Timing errors are difficult to detect with the naked eye.
Your upper body also contributes to running efficiency, and poor upper body mechanics can also play a role in knee pain.
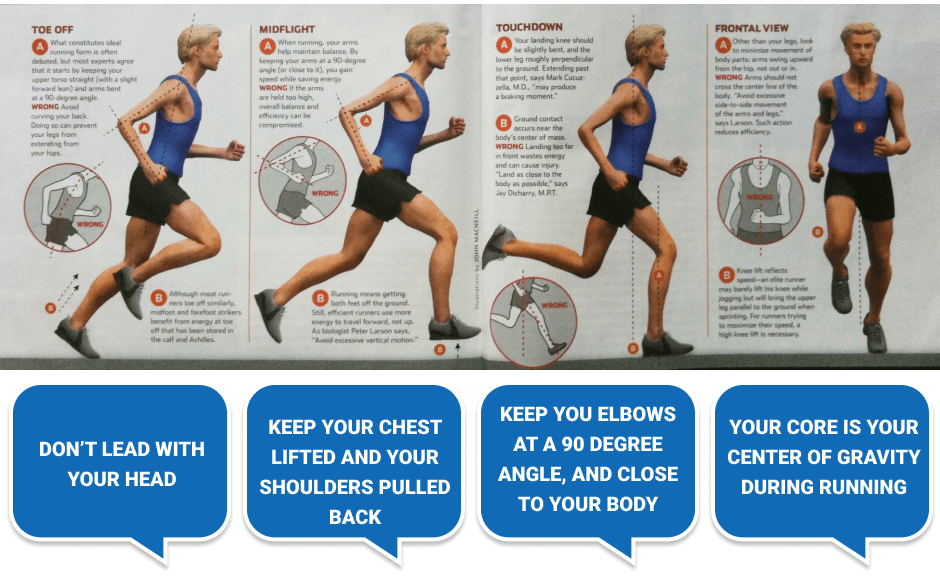
Following are a few pointers for upper body alignment and engagement to optimize running performance:
Don’t lead with your head. Keep your chin parallel to the ground and your gaze forward, ears aligned with your shoulders.
Keep your chest lifted and your shoulders pulled back. Move your shoulders independently of your torso, and avoid shrugging as you get tired. Your shoulders should move opposite to one another, and in line with the contralateral leg. In other words, the right shoulder moves forward with the left leg, and vice versa.
Keep you elbows at a 90 degree angle, and close to your body. Swing each arm forward with the opposite leg, fists traveling from chin to hip to help you propel forward. Keep your hands relaxed to conserve energy.
Your core is your center of gravity during running, and you should contract your core muscles as you run. Your pelvis and torso should shift slightly from side to side, to keep your weight over the stance leg. Your torso should hinge forward slightly over your hips to maximize power and momentum from your gluteus maximus.
The best way to prevent and treat runner’s knee is to identify mechanical deficiencies and correct your gait. NYDNRehab provides chiropractic care and physical therapy in Manhattan. Our gait analysis and retraining lab offers some of the most advanced technologies and innovative training approaches in the United States.
Our state-of-the-art gait lab features:
Whether you are a novice runner or an elite athlete, running gait analysis and retraining can make a world of difference in how well and how long you run.
Dixit, Sameer, et al. “Management of patellofemoral pain syndrome.” Am Fam Physician 75.2 (2007): 194-202.
Novacheck, Tom F. “The biomechanics of running.” Gait & posture 7.1 (1998): 77-95.
Sinclair, J., and James Selfe. “Sex differences in knee loading in recreational runners.” Journal of biomechanics 48.10 (2015): 2171-2175.

Verified Expert Profiles
Dr. Lev Kalika is a world-recognized expert in musculoskeletal medicine. with 20+ years of clinical experience in diagnostic musculoskeletal ultrasonography, rehabilitative sports medicine and conservative orthopedics. In addition to operating his clinical practice in Manhattan, he regularly publishes peer-reviewed research on ultrasound-guided therapies and procedures. He serves as a peer reviewer for Springer Nature.
Dr. Kalika is an esteemed member of multiple professional organizations, including:
Below is a prime example of how ultrasound can take the guesswork out of diagnosis.

A bad physical therapy experience is one of the primary causes of unnecessary surgery
In this instance, an athlete was originally diagnosed with minor quadriceps muscle strain and was treated for four weeks, with unsatisfactory results. When he came to our clinic, the muscle was not healing, and the patients’ muscle tissue had already begun to atrophy.
Upon examination using MSUS, we discovered that he had a full muscle thickness tear that had been overlooked by his previous provider. To mitigate damage and promote healing, surgery should have been performed immediately after the injury occurred. Because of misdiagnosis and inappropriate treatment, the patient now has permanent damage that cannot be corrected.
The most important advantage of Ultrasound over MRI imaging is its ability to zero in on the symptomatic region and obtain imaging, with active participation and feedback from the patient. Using dynamic MSUS, we can see what happens when patients contract their muscles, something that cannot be done with MRI. From a diagnostic perspective, this interaction is invaluable.
Dynamic ultrasonography examination demonstrating
the full thickness tear and already occurring muscle atrophy
due to misdiagnosis and not referring the patient
to proper diagnostic workup
Demonstration of how very small muscle defect is made and revealed
to be a complete tear with muscle contraction
under diagnostic sonography (not possible with MRI)

Complete tear of rectus femoris
with large hematoma (blood)

Separation of muscle ends due to tear elicited
on dynamic sonography examination










































